

Forearm fracture account for a good number of orthopedic emergencies. The anatomy of the forearm is unique as there are two bones that have to work in coordination to allow elbow and wrist function. The alignment of these two bones aka radius and ulna; is important for twisting function of forearm e.g. while turning a key. These days forearm fractures at most age groups are managed by surgery – plate fixation.
There is a complex arrangement of nerves and vessels around the two bones in the forearm. For a good result of surgery, the structure must protect from any iatrogenic damage.
Nerve of Forearm
Therefore, most of the surgical approaches to bones of the forearm are design in a way to avoid handling of vital structures. However, the upper part of radius remains an area still involving handling of an important nerve: posterior interosseous nerve of forearm. This nerve plays a crucial role in movement of the wrist. The approach commonly used involves dissecting the nerve out and then doing the plating. This subjects the nerve to a lot of handling and carries a risk of nerve damage.
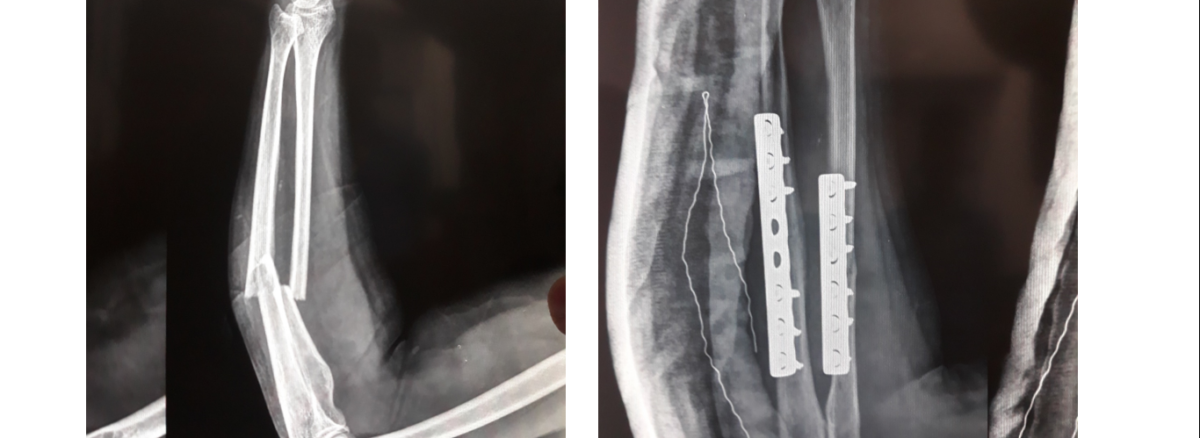
Forearm Fracture Case
We present case of a young laborer, who suffered fracture if both bones of forearm at workplace. After initial management, the patient was taken up for surgery. Both the fractures stabilizes with plates. However, the upper part of radius approached differently. Herein, the nerve is not dissect out. Rather the muscle mass; in which the nerve is embedd; is lift en-mass off the bone. The muscle itself protected the nerve from damage and allowed a decent exposure of bone to allow fixation. In the post op period, the patient is evaluate clinically for good nerve function and discharged in satisfactory condition. The approach commonly used involves dissecting the nerve out and then doing the plating. This subjects the nerve to a lot of handling and carries a risk of nerve damage.